Healthcare Software Development Cost in the Middle East
A Complete Enterprise Guide for Hospitals, Healthcare Startups, Pharma Companies, and Digital Health Innovators Across the GCC. This comprehensive guide explores healthcare software development costs across the GCC, including the UAE, Saudi Arabia, Qatar, Bahrain, Kuwait, and Oman. It covers software categories such as telemedicine, EHR systems, AI healthcare applications, digital therapeutics, and remote patient monitoring platforms. The guide also examines regulatory frameworks including UAE PDPL, Saudi PDPL, NPHIES, DHA requirements, and PMDA considerations, while providing real-world GCC case studies, development timelines, hidden costs, ROI expectations, and future healthcare technology trends shaping the region in 2026 and beyond.

Key Takeaways
- GCC healthcare is moving from digital transformation to digital infrastructure, with governments investing heavily in AI, telemedicine, smart hospitals, and connected healthcare ecosystems.
- Healthcare software development costs in the GCC range from USD 40,000 for basic telemedicine platforms to over USD 2 million for enterprise AI-powered healthcare and Digital Therapeutics platforms.
- Compliance is one of the largest cost drivers, with regulations such as UAE PDPL, Saudi PDPL, NPHIES, DHA requirements, and international frameworks significantly impacting architecture and development decisions.
- AI healthcare platforms require additional investments in data annotation, model training, clinical validation, explainability, and continuous monitoring, making them more complex than traditional healthcare applications.
- Interoperability is no longer optional. Modern healthcare platforms must integrate with EHRs, laboratories, pharmacies, insurance systems, medical devices, and national health exchanges.
- Remote Patient Monitoring (RPM), Digital Therapeutics (DTx), AI Clinical Decision Support, and Smart Hospital initiatives are among the fastest-growing healthcare technology segments across the GCC.
- Hidden costs such as cybersecurity audits, cloud infrastructure, AI model maintenance, training, compliance updates, and post-launch optimization can significantly impact total project budgets.
- Organizations that incorporate compliance, security, interoperability, and scalability from the beginning avoid costly redesigns and accelerate deployment timelines.
The Middle East is rapidly becoming one of the world's most ambitious healthcare innovation regions. Across Saudi Arabia, the UAE, Qatar, Bahrain, Kuwait, and Oman, governments are investing billions of dollars to modernize healthcare infrastructure, improve patient outcomes, increase system efficiency, and accelerate digital transformation at a scale that few regions are attempting simultaneously.
Healthcare organizations are moving well beyond simple digitization initiatives. They are investing in intelligent, connected healthcare ecosystems powered by artificial intelligence, remote patient monitoring, Internet of Medical Things, telemedicine, clinical decision support systems, digital therapeutics, blockchain-secured data integrity, health information exchanges, precision medicine, and genomics platforms.
As healthcare systems become increasingly connected, software is evolving from a support function into critical national healthcare infrastructure. Yet despite this rapid transformation, one question continues to dominate boardroom discussions and investment planning sessions:
How much does healthcare software development actually cost in the Middle East?
A simple patient appointment scheduling application may cost less than USD 50,000. A PMDA-ready remote patient monitoring platform, an AI-powered clinical decision support system, or an integrated hospital intelligence ecosystem can exceed USD 1.5 million. The answer depends on far more than development effort alone.
Modern healthcare software costs in the GCC are shaped by regulatory compliance obligations, clinical safety requirements, cybersecurity architecture mandates, data interoperability standards, AI validation requirements, medical device certification pathways, long-term maintenance obligations, and the operational realities of deploying complex systems across healthcare networks that serve millions of patients.
This guide explores the true cost of healthcare software development in the GCC, what drives those costs, real market case studies, expected ROI, emerging technology trends, and how healthcare organizations can invest strategically in 2026 and beyond.
Why Healthcare Technology Investment Is Accelerating Across the GCC
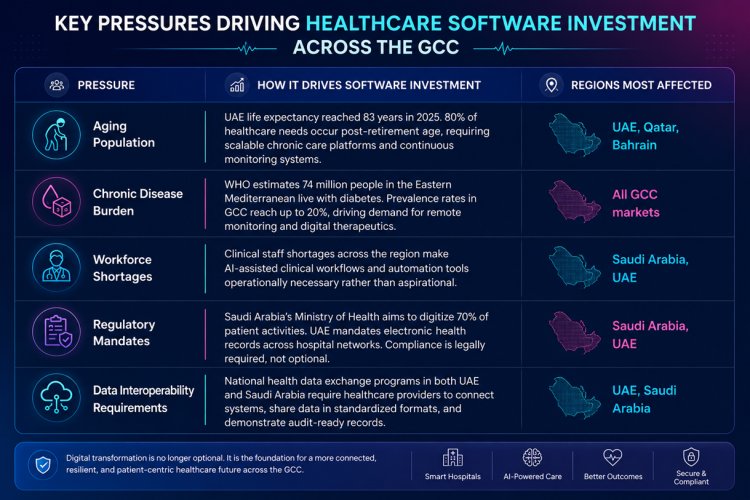
The Aging Population Challenge
Healthcare demand is increasing significantly across the GCC. The UAE's life expectancy now exceeds 83 years, ranking among the highest globally. Saudi Arabia's population aged 60 and above is projected to grow substantially over the coming decades, driven by improvements in healthcare quality and rising life expectancy across the Kingdom.
As populations age, healthcare systems face growing demand for chronic disease management, long-term care coordination, home-based healthcare delivery, continuous remote monitoring, and highly personalized treatment plans. Traditional hospital-centric care models struggle to scale sustainably under these conditions. Digital healthcare technologies provide the pathway to efficient, connected, and scalable healthcare delivery at the population level.
Rising Chronic Disease Burden
The Middle East continues to experience some of the highest prevalence rates globally for diabetes, hypertension, obesity, and cardiovascular disease. WHO estimates that 74 million people in the Eastern Mediterranean region live with diabetes. Prevalence rates in GCC countries reach as high as 20% of the adult population in some markets, creating an urgent demand for continuous care models rather than episodic clinical visits.
This chronic disease burden is driving substantial investment in remote patient monitoring platforms, AI-powered predictive analytics that identify deteriorating patients before hospitalization, digital therapeutics for long-term behavioral intervention, and connected healthcare devices that extend clinical visibility into the patient's home environment.
Healthcare Workforce Challenges
Healthcare providers across the GCC face growing and compounding workforce pressures. Clinician shortages, significant administrative documentation burden, increasing patient volumes, and constrained training pipelines are creating operational sustainability challenges at hospital networks across the region. Technology is being deployed not to replace clinical judgment, but to automate administrative workflows, reduce documentation burden, improve care coordination across facility networks, and enhance clinical decision-making through data-driven intelligence tools.
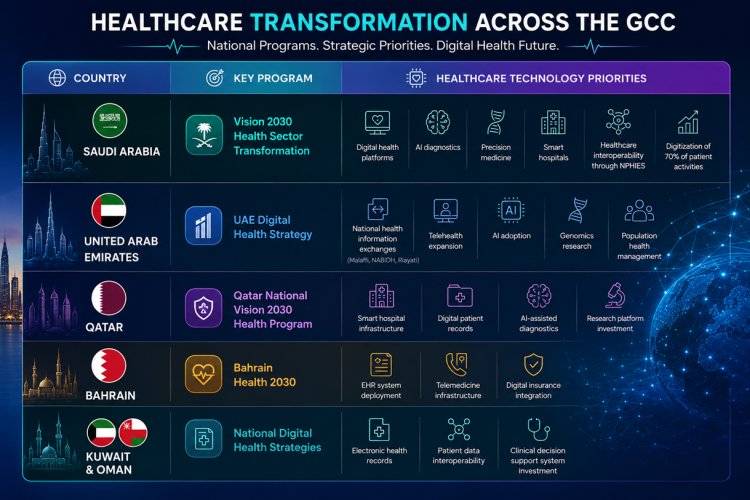
Government-Led Digital Transformation Programs
The most powerful driver of healthcare technology investment across the GCC is direct government mandate and financial commitment. These are not advisory frameworks. They are funded, structured transformation programs with measurable targets and regulatory enforcement mechanisms.
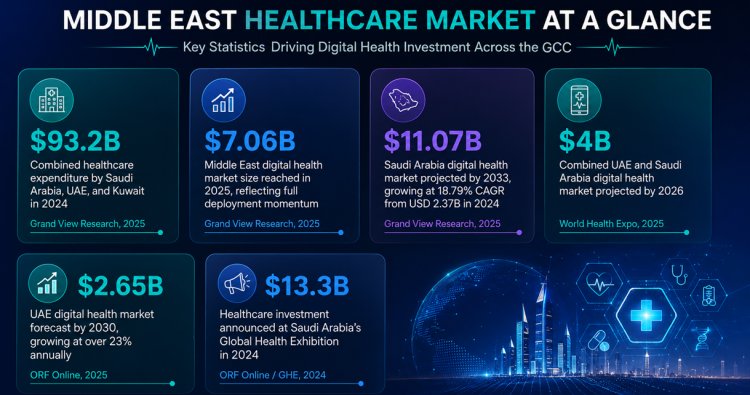
The GCC Healthcare Technology Market
The scale of healthcare technology investment across the GCC makes the compliance, architecture, and interoperability requirements that shape software development costs easier to understand. These are not niche markets with experimental budgets. They are nationally funded digital infrastructure programs measured in billions of dollars.
Healthcare Software Categories and Development Costs
The category of software being built is the single most significant factor determining development cost. A telemedicine platform and an AI-powered digital therapeutics system are both healthcare software, but they have almost nothing in common from a cost, compliance, or engineering complexity perspective.
The following categories represent the primary software types Interakt TechSol develops for healthcare clients across the GCC and Asia-Pacific markets:

Detailed Cost Comparison by Project Type
| Software Type | USD Range | AED Range | Timeline | Complexity | Compliance Level |
|---|---|---|---|---|---|
| Telemedicine Platform | USD 40K to 150K | AED 147K to 551K | 3 to 6 months | Moderate | DHA basic |
| EHR System | USD 100K to 500K | AED 367K to 1.84M | 6 to 18 months | High | NPHIES, PDPL |
| Remote Patient Monitoring | USD 120K to 750K | AED 441K to 2.75M | 6 to 15 months | High | IoMT + PDPL |
| AI Healthcare Platform | USD 150K to 1.5M | AED 551K to 5.5M | 8 to 24 months | Very High | SaMD, DHA, PMDA |
| Digital Therapeutics | USD 250K to 2M | AED 918K to 7.34M | 12 to 24 months | Enterprise | Full regulatory pathway |
* AED figures calculated at the 2026 rate of approximately 3.67 AED per USD. Cost ranges reflect GCC market conditions. AI-intensive and SaMD-regulated platforms consistently sit at the upper end of or above these ranges due to data preparation, validation, and regulatory certification requirements.
What Actually Drives Healthcare Software Development Costs
Many organizations begin healthcare technology projects with incorrect assumptions about where budget goes. Feature count and screen count are minor variables. The true cost drivers are structural requirements that apply regardless of which features are chosen.
- Regulatory Compliance: UAE PDPL, Saudi PDPL, NPHIES integration standards, DHA licensing, and PMDA SaMD certification each impose architecture constraints and validation obligations. Compliance requirements that are identified during development cost significantly more to address than those built in from day one. (15% - 30% of total project cost)
- Data Security Architecture: Healthcare remains one of the highest-value targets for cyberattacks globally. End-to-end encryption, identity and access management, immutable blockchain audit trails, vulnerability testing, and continuous security monitoring are non-negotiable. (10% - 20% of total project cost)
- AI Development and Validation: AI healthcare projects require data collection, annotation, model training, clinical validation, explainability documentation for regulatory review, and ongoing model monitoring pipelines. (25% - 40% of AI project cost)
- System Integration and Interoperability: Healthcare software rarely operates in isolation. Integration with EHR systems, laboratory platforms, imaging networks, pharmacy systems, insurance platforms, NPHIES, and government health data exchanges is typically required. (20% - 40% of total project cost)
- UX for Clinical Environments: Clinical staff, patients, administrators, insurance teams, and compliance officers each require distinct interfaces. Arabic-English bilingual UX with full RTL support adds significant design effort. Poor UX is among the highest post-launch cost drivers due to retraining and low adoption. (10% - 20% of total project cost)
- Regional Infrastructure Requirements: UAE and Saudi Arabia impose data residency requirements restricting where patient data is processed and stored. GCC-hosted regional cloud infrastructure, disaster recovery environments, and high-availability architecture for clinical systems carrying patient safety obligations add ongoing infrastructure cost from go-live day. (Ongoing at 15% - 25% annually)
Regulatory and Compliance Landscape Across GCC Markets
Regulatory alignment in GCC healthcare is not a documentation exercise completed before launch. It is a foundational architecture constraint that shapes infrastructure choices, data model design, access control structures, audit trail requirements, and clinical validation obligations from the first planning session. Organizations that treat compliance as a late-stage checklist consistently encounter the most expensive and disruptive project corrections.
| Framework | Jurisdiction | Core Requirements for Healthcare Software | Architecture Implications |
|---|---|---|---|
| UAE PDPL (effective 2023) | United Arab Emirates | Lawful basis for data processing, data subject rights management (access, correction, erasure), 72-hour breach notification, restrictions on cross-border data transfer without adequate protection. | UAE-hosted infrastructure required, consent management system, data subject request workflow automation, breach response system. |
| Saudi PDPL | Kingdom of Saudi Arabia | Explicit consent required for sensitive health data, data localization mandating Saudi-hosted infrastructure, NDMO compliance framework, penalties for unauthorized data disclosure. | Saudi-hosted cloud deployment, granular consent tracking, data classification and tagging architecture, NDMO audit trail readiness. |
| NPHIES | Kingdom of Saudi Arabia | Mandatory integration for all healthcare providers and insurance companies. Standardized data formats for claims submission, eligibility verification, and clinical data exchange using HL7 FHIR standards. | NPHIES-compliant API integration, HL7 FHIR implementation, real-time eligibility checking, claims processing workflow. |
| DHA and DOH | UAE (Emirate level) | Software as a Medical Device classification and licensing, clinical safety requirements, data privacy standards aligned with ADHICS, technical documentation for software-based medical tools. | SaMD risk classification documentation, clinical workflow safety validation, authority technical file preparation and submission management. |
| PMDA SaMD | Japan (for Japan-facing platforms) | Class II Software as a Medical Device certification, quality management system implementation, clinical evidence documentation, post-market surveillance program, intended use specification in Japanese regulatory format. | Full QMS implementation, clinical evidence data collection, post-market surveillance workflow, technical file in PMDA-required format. |
| Malaffi and NABIDH | Abu Dhabi & Dubai, UAE | Connectivity to UAE health information exchange networks, SNOMED CT and LOINC coding standards, real-time patient record sharing across public and private facilities. | HL7 FHIR API integration, standardized clinical coding, real-time record synchronization architecture. |
Interakt TechSol's certified experience: Interakt TechSol has direct experience with PMDA Class II SaMD certification through the Impakt Health platform. This gives our healthcare development teams first-hand regulatory knowledge that most GCC technology vendors cannot offer.
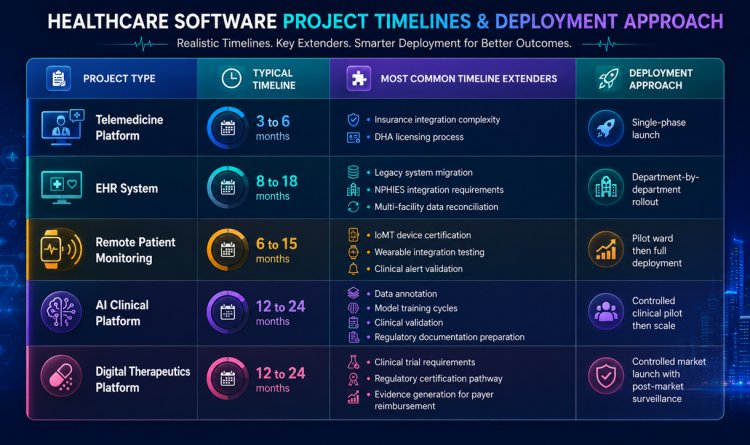
Development Timeline and Deployment Approach
- Discovery and Compliance Planning (4 to 8 weeks): Regulatory gap analysis, clinical workflow mapping, legacy system audit, compliance framework identification, stakeholder alignment across clinical, IT, legal, and compliance teams. Rushing discovery is the primary cause of expensive rework.
- UI and UX Design (4 to 10 weeks): Role-specific interface design for clinical staff, patients, administrators, and compliance teams. Arabic-English bilingual UX with full RTL support. Mobile-first design for patient-facing applications.
- Core Platform Development (3 to 12 months): Backend engineering, including AI model integration and training pipelines, blockchain audit trail implementation, IoMT connectivity, EHR integration, insurance and billing system connectivity, and security architecture implementation.
- Integration and Interoperability (1 to 4 months): Connection with existing EHR systems, laboratory platforms, imaging networks, NPHIES or equivalent national health data exchanges.
- Testing, Validation, and Regulatory Review (1 to 3 months): Clinical workflow testing under realistic operational conditions. AI model performance validation with real clinical data sets. Security penetration testing and clinical evidence documentation preparation.
- Deployment and Clinical Stabilization (2 to 6 weeks per phase): Phased rollout by department, ward, facility, or geography to protect patient care continuity. Structured onboarding in Arabic and English.
Typical Total Timeline by Project Type
Hidden Costs Most Healthcare Organizations Miss
Healthcare technology projects consistently exceed budgets not because of unexpected feature requests, but because entire cost categories were never included in the initial plan. These are operational costs that begin the moment a platform goes live in a clinical environment:
- Clinical Validation: AI applications, digital therapeutics, and SaMD platforms require clinical testing with real patient populations before regulatory approval. (USD 30,000 to 250,000+)
- Cloud Infrastructure: GCC data residency requirements mandate regional hosting. Disaster recovery environments, backup systems, monitoring infrastructure, and high-availability configurations add measurable ongoing cost. (AED 22,000 to 110,000 annually)
- Cybersecurity Audits: Annual penetration testing, vulnerability assessments, smart contract audits for blockchain components, and third-party security reviews are required. (AED 30,000 to 90,000 per cycle)
- AI Model Maintenance: Healthcare AI models drift as patient populations and clinical practices evolve. Retraining cycles and performance monitoring are ongoing engineering obligations. (15% to 25% of build cost annually)
- Software Maintenance: Bug fixes emerging from real clinical usage, feature refinements driven by clinician feedback, and platform updates triggered by regulatory framework changes are standard recurring costs. (15% to 25% of build cost annually)
- Training and Change Management: Initial onboarding and refresher sessions for clinical, administrative, and compliance teams in both Arabic and English. (AED 15,000 to 60,000 per cycle)
- Post-Launch Optimization: UX refinements, additional integrations, and system tuning in the first 12 months post-launch are standard in enterprise healthcare deployments. (AED 30,000 to 120,000 in year one)
- Regulatory and Legal Updates: GCC healthcare regulations continue to evolve. Legal review of data processing agreements and compliance documentation maintenance are ongoing. (AED 20,000 to 75,000 annually)
Real GCC Healthcare Digital Transformation Case Studies
Case Study 1: Seha Virtual Hospital
Jurisdiction: Saudi Arabia · Ministry of Health · Telemedicine at National Scale
Challenge: Providing equitable specialist healthcare access across a geographically vast country with significant regional disparities in clinical specialist availability. Physical travel burden for rural and remote populations limited access to specialist care.
Solution: A national virtual hospital infrastructure launched in February 2022, connecting patients across Saudi Arabia with specialist clinical teams through a centralized virtual care platform integrated with the national Sehhaty mobile application.
Technology Stack: Telemedicine platform, national health information exchange integration, AI-assisted clinical support tools, IoT-enabled remote monitoring, digital clinical research platform. Connected 200+ hospitals and 2,000+ health centers.
- 16M+: Virtual appointments delivered in 2025
- 56%: Growth in virtual appointments YoY
- 220K+: Clinical cases managed through virtual care
- 51M+: Total appointments since inception through 2024
Case Study 2: Malaffi
Jurisdiction: Abu Dhabi, UAE · Department of Health · MENA's First Health Information Exchange
Challenge: Highly fragmented patient records across 3,000+ healthcare facilities and 90+ distinct electronic medical record systems in Abu Dhabi. Clinicians lacked access to complete patient history at point of care, leading to duplicated tests.
Solution: The MENA region's first Health Information Exchange platform, connecting public and private healthcare providers across Abu Dhabi through a unified, secure, real-time patient record sharing infrastructure. Implemented SNOMED CT and LOINC standards at scale.
Technology Stack: Health information exchange platform, HL7 FHIR integration across 83 unique EMR systems, SNOMED CT and LOINC coding standardization, AI-driven clinical analytics, radiology image exchange, real-time data synchronization.
- 3.5B: Clinical records reached by Aug 2025
- 12.7M: Unique patient profiles connected
- 53,476: Authorized clinical users across facilities
- 83: Unique EMR systems connected natively
Case Study 3: NPHIES
Jurisdiction: Saudi Arabia · National Health Platform · Insurance and Clinical Data Interoperability
Challenge: Insurance claims processing fragmentation, high administrative overhead for healthcare providers managing multiple insurance systems, and lack of standardized clinical data exchange between healthcare facilities and payers across Saudi Arabia.
Solution: A mandatory national health information and insurance exchange platform requiring integration by all licensed healthcare providers and insurance companies in Saudi Arabia. Standardized HL7 FHIR-based data formats for claims, eligibility, and clinical information exchange.
Impact on Software Development: Every healthcare software platform operating in Saudi Arabia must now include NPHIES integration as a core technical requirement. This single compliance obligation adds 15 to 25% to development cost and timeline for any clinical platform in the Saudi market.
ROI of Healthcare Software Development
| Software Category | Primary ROI Drivers | Measurable Outcomes | Typical ROI Timeline |
|---|---|---|---|
| Telemedicine Platform | Reduced facility overhead per consultation, geographic expansion, improved patient retention through convenience. | Lower cost per consultation, increased patient volume capacity, reduced no-show rates. | 12 to 18 months |
| EHR System | Clinical documentation time reduction, elimination of duplicate test ordering, insurance claim accuracy, audit readiness. | 30 to 50% reduction in clinical admin time, faster insurance claim processing, improved compliance outcomes. | 18 to 24 months |
| Remote Patient Monitoring | Hospital readmission reduction for chronic disease patients, early clinical intervention through predictive alerts. | 20 to 35% reduction in preventable readmissions, earlier clinical escalation, lower cost per chronic episode. | 18 to 36 months |
| AI Healthcare Platform | Diagnostic accuracy improvement, clinical workflow automation, reduced diagnostic delay, workforce augmentation. | Faster time to diagnosis, reduced diagnostic error rate, improved resource allocation across departments. | 24 to 36 months |
| Digital Therapeutics | Long-term chronic disease management cost reduction, patient adherence improvement, payer reimbursement validation. | Improved medication adherence, reduced disease progression costs, payer reimbursement activation. | 36 to 48 months |
Healthcare Technology Trends Driving Investment in 2026
The investment thesis for healthcare technology in the GCC has shifted. Organizations are no longer funding the digitization of paper processes. They are investing in intelligent, connected, and data-driven healthcare ecosystems that generate measurable clinical and operational value.
- AI-Powered Diagnostics and Clinical Support: AI is actively assisting clinicians in radiology, pathology, oncology, and rare disease detection across GCC hospitals. Government investment in AI data centers in Saudi Arabia and the UAE is accelerating clinical AI deployment at scale.
- Hospital-to-Home Care Transformation: Remote patient monitoring adoption is shifting care delivery away from hospital-centric models toward continuous home-based monitoring for chronic conditions. IoT-enabled vital sign tracking and AI-driven alert systems are central to this transition.
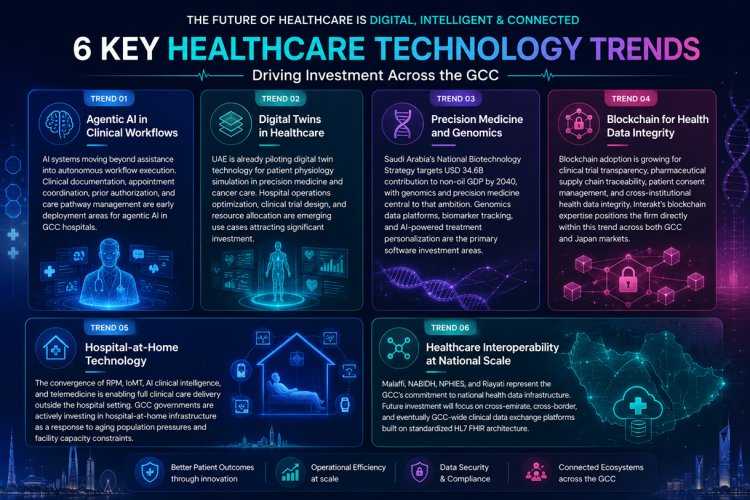
- Digital Twins in Healthcare Operations: UAE is piloting digital twin technology for patient physiology simulations and precision medicine. Hospital operations, resource optimization, and clinical trial design are all emerging use cases for digital twin platforms in the GCC.
- Blockchain for Healthcare Data Integrity: Blockchain adoption in healthcare is growing for clinical trial transparency, pharmaceutical supply chain traceability, patient consent management, and health data integrity across multi-provider networks. Interakt's expertise in blockchain-enabled healthcare ecosystems positions it at the center of this trend.
- Smart Hospitals and IoMT Integration: Saudi Arabia's smart hospital market is projected to grow from USD 674 million in 2024 to USD 1.77 billion by 2033. Connected medical devices, AI-assisted surgical systems, 5G-enabled remote monitoring, and automated clinical workflow tools are core infrastructure investments.
Precision Medicine and Genomics Platforms: The UAE is integrating genomics data into cancer research through partnerships such as the Abu Dhabi Department of Health and GSK collaboration. Saudi Arabia's National Biotechnology Strategy envisions a USD 34.6 billion contribution to non-oil GDP by 2040, with precision medicine at the center.
How to Reduce Healthcare Software Development Costs Without Sacrificing Quality
| Strategy | How It Works in Healthcare Contexts | Typical Saving | Best Applied At |
|---|---|---|---|
| Start with a validated MVP | Focus the first release on solving one core clinical or operational problem. Reduces initial investment while validating product-market fit. | 30 to 50% of initial spend | Before architecture is finalized |
| Build modular architecture | Independent modules for clinical workflows, billing, analytics, and compliance allow isolated upgrades and lower lifetime maintenance overhead. | 15 to 30% lower lifetime maintenance | Architecture design phase |
| Prioritize interoperability in architecture | Integration planning during the architecture stage prevents redesigns when connecting with EHR systems, NPHIES, or insurance platforms. | Avoids AED 100K to 400K redesign | Discovery and architecture phase |
| Invest in data quality before AI | Organizations that invest in data governance, annotation, and quality management before model development achieve significantly lower long-term costs. | Prevents complete AI rebuilds | Before AI model development begins |
| Plan compliance in architecture | UAE PDPL, Saudi PDPL, NPHIES, and DHA requirements built into architecture from the start cost a fraction of what compliance retrofitting costs. | Avoids project stoppage and full redesign | Discovery phase, before any code is written |
Interakt TechSol's approach: We begin every healthcare engagement with a structured compliance and architecture discovery session before any development decisions are made. This single session has prevented expensive compliance redesigns across multiple GCC healthcare deployments and consistently brings projects in on budget and on timeline.
Why Choose Interakt TechSol
| Capability Area | What We Deliver |
|---|---|
| Healthcare Software Development | EHR systems, patient management platforms, hospital information systems, clinical workflow automation, multi-facility data synchronization. |
| AI and Machine Learning | Clinical decision support, medical imaging analysis, disease risk prediction, population health analytics, NLP for clinical documentation. |
| Remote Patient Monitoring | IoMT device integration, wearable connectivity, real-time vital sign monitoring, AI-driven clinical alerting, hospital-to-home care platforms. |
| Blockchain for Healthcare | Health data integrity systems, clinical trial transparency platforms, pharmaceutical supply chain traceability, patient consent management. |
| IoT and Connected Healthcare | IoMT integration, wearable device connectivity, smart monitoring systems, edge computing for clinical data processing. |
| Regulatory Navigation | SaMD certification support, compliance architecture design, regulatory documentation preparation, post-market surveillance system implementation. |

FAQ
How much does healthcare software development cost in the UAE?
Most healthcare software projects in the UAE range from USD 40,000 for a basic telemedicine application to USD 2 million or more for a full digital therapeutics or AI clinical platform. The wide range reflects the difference between a single-function patient-facing app and an enterprise-grade, regulatory-certified, multi-facility system. Compliance requirements, integration depth, and AI component complexity are the variables that move the number most significantly within that range.
How long does healthcare software development take in the Middle East?
Projects typically take between 3 and 24 months, depending on software category and regulatory scope. Telemedicine platforms with standard features can be delivered in 3 to 6 months. EHR systems, remote patient monitoring platforms, and AI clinical applications require 6 to 24 months. The most common causes of timeline extension are regulatory approval processes, clinical validation requirements, and legacy system integration complexity, not development speed.
Is AI healthcare software significantly more expensive to build?
Yes, substantially. AI projects require data collection, annotation, model training, clinical validation, explainability documentation, and ongoing monitoring pipelines. These are separate from standard software development activities and add meaningful cost and time. AI model maintenance (15 to 25% of build cost annually) and retraining cycles are ongoing obligations that must be budgeted before a project begins. Despite the higher cost, well-implemented clinical AI consistently delivers measurable ROI through diagnostic accuracy improvements, workflow automation, and reduced clinical error rates.
What is the most expensive component of enterprise healthcare software in the GCC?
For enterprise healthcare platforms, interoperability and regulatory compliance are typically the largest combined cost drivers, accounting for 35 to 60% of total project investment when properly scoped. Integration with national health data exchanges such as NPHIES, legacy EHR systems, insurance platforms, and laboratory networks introduces complexity that requires specialized senior architecture planning.